
The Lead II rhythm strip shown below in Figure 1 was obtained was obtained from a patient during cardiopulmonary resuscitation. It is a follow-up tracing to our ECG Blog Review #19. The patient was hypotensive at the time Figure 1 was recorded. Does the rhythm represent 2nd degree AV Block, Mobitz Type II? How to proceed clinically?
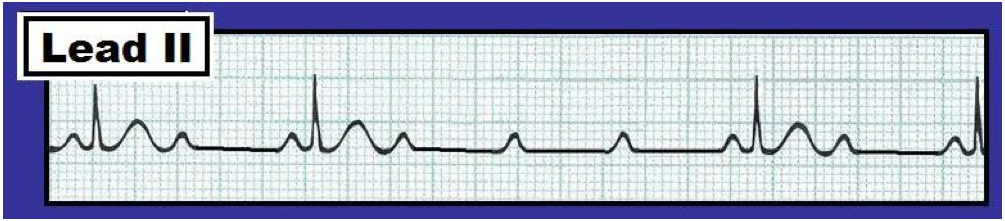 |
| Figure 1 - Lead II rhythm strip from a patient in cardiac arrest. Is this 2nd degree AV block, Mobitz Type II? |
INTERPRETATION: The ventricular rhythm in Figure 1 is slow and irregular. Nevertheless – the QRS complex is narrow, and the atrial rate is regular at ~115/minute. The P waves immediately preceding each QRS complex manifest a fixed (and normal) PR interval. Thus, these P waves are conducting. This means that the rhythm is not complete AV block. Since there are many non-conducted P waves on the tracing – the rhythm must represent some form of high-grade 2nd degree AV block.
-----------------------------------------------------
As discussed in ECG Blog Review #19 – Second degree AV blocks are generally classified into one of 3 types:
- Mobitz I (AV Wenckebach) – in which the PR interval progressively lengthens until a beat is dropped. This is by far the most common form of 2nd degree AV block.
- Mobitz II – in which there is a constant PR interval for consecutively conducted beats until one or more beats are dropped.
- 2-to-1 AV Block – in which every-other-P-wave is conducted. Because one never sees two consecutively conducted beats – you can not tell if the PR interval is lengthening or not. As a result – it is impossible to know for sure whether this form of 2nd degree AV block represents Mobitz I or Mobitz II.
-----------------------------------------------------
Returning to this Case: There are features of both Mobitz I (AV Wenckebach) and Mobitz II on the tracing shown in Figure 1. In favor of Mobitz II is the low conduction ratio and high grade of AV block. No less than 3 P waves in a row are non-conducted in the middle of the tracing. However, the QRS complex is narrow – which is highly unusual for Mobitz II.
- Clinically – the importance of distinguishing AV Wenckebach (Mobitz I) from Mobitz II relates to the much better prognosis of Mobitz I, a generally better response to treatment with Atropine, and a much lower likelihood of needing a pacemaker. That said – it is impossible to be certain which form of 2nd degree AV block is present from the tracing in Figure 1 alone, since one never sees two P waves in a row that conduct. Thus, one can not tell if the PR interval is progressively increasing until the point of non-conduction. Although unusual for Mobitz I – more than one P wave in a row may be blocked on occasion with this conduction disturbance. From a practical treatment perspective, however – distinguishing between Mobitz I and Mobitz II appears to be less important since a pacemaker may be needed in either case unless the high-grade degree of AV block improves.
-----------------------------------------------------
FINAL (Advanced) PEARL: Even though far fewer P waves are conducted in Figure 1 from this Blog post (above) compared to the rhythm strip showing 2-to-1 AV conduction in Figure 1 from ECG Blog Review #19 (We reproduce that 2:1 AV block tracing below) – the “degree” of AV block per se has not necessarily “worsened”. Why not? HINT: Has the atrial rate changed in the two tracings?
 |
| Figure 1 from ECG Blog Review #19 - Lead II rhythm strip showing 2:1 AV block. |
ANSWER: The atrial rate in Figure 1 of this Blog post (at the top of this page) is now faster (~115/minute) than it was when there was 2:1 AV conduction (Note the P-P interval in Figure 1 from Blog Review #19 = 3 large boxes = an atrial rate of 100/minute). Rather than “worsening” of the degree of AV block per se – the lower conduction rate may simply be the result of the faster atrial rate. Treatment of 2nd degree AV block with atropine may at times be a double-edged sword. It may improve the situation (by facilitating conduction through the AV node) – but it can at times worsen the situation by increasing the atrial rate by an amount that may be too fast to conduct. Bottom Line: We suspect that Figure 1 in this Blog post (at the top of this page) represents high-grade 2nd degree AV block, Mobitz Type I – because the QRS is narrow, and Mobitz I is by far the most common form of 2nd degree AV block. Even though treatment with atropine was appropriate (since this drug is often effective for Mobitz I) – atropine paradoxically worsened the situation in this case, because it further increased the atrial rate. Temporary pacing is indicated given bradycardia with hypotension.
------------------------------
during cardiopulmonary resuscitation that means the patient coded....So during CPR if we get such a rhythm, is atropine indicated?? or do we continue with our usual steps of ACLS???? Or is this a situation during ROSC???
ReplyDelete@ MG — The answer is given in the last 2 sentences — :)
Delete