
- How would you interpret her ECG?
- How might you explain the finding of normal coronary arteries on cardiac catheterization?
 |
| Figure 1: ECG obtained from a 74-year old woman with renal colic, but no chest pain. |
- Assessment of Q-R-S-T Changes is remarkable for the presence of inferior Q waves — normal transition (R wave becoming taller than the S wave between leads V3-to-V4) — and ST segment coving with marked elevation in the inferior leads. This is accompanied by deep T wave inversion.
- Similar abnormal ST segment coving and elevation (albeit not as marked) is also present in leads V4,V5. Deep, symmetric T wave inversion that begins in lead V3 is seen in V4,V5.
- Takotsubo Cardiomyopathy is an underappreciated cause of acute ECG abnormalities and new-onset heart failure. The entity was first described in Japan in 1990, with the name takotsubo being derived from a specially designed container used by Japanese fishermen to trap octopuses. The unusual round bottom and narrow neck design of takotsubo resembles the diagnostic picture on cardiac catheterization obtained as a result of ballooning of the cardiac apex with hypercontraction of the base (Figure-2).
- Other names attributed to this entity include “stress cardiomyopathy” and “broken-heart syndrome” — in reference to the common occurrence of severe physical or emotional stress prior to onset of the disorder. Awareness of this syndrome is important — because the initial ECG may mimic a large apical infarction (with inferior and anterior ST segment elevation). Transient heart failure is common during the initial stages, but fortunately resolves within a few weeks in most cases.
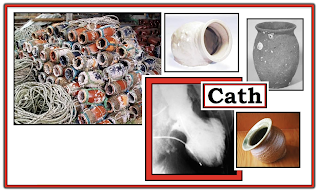 |
| Figure-2: Collection of actual takotsubo showing the round bottom and narrow neck — that resembles the diagnostic picture seen on the cardiac catheterization ventriculogram (shown here during end-systole). Note characteristic "ballooning of the apex and hypercontractility of the base during cardiac cath (See text). |
The precise mechanism for Takotsubo CMP remains elusive. While factors such as coronary spasm; disturbance of the microcirculation; coronary artery anatomic variation; and neurogenic myocardial stunning have all been implicated — their role is uncertain. What has been shown — is that abnormal response to an increase in endogenous catecholamines is almost always involved. Blood epinephrine and norepinephrine levels are unmistakably elevated (sometimes dramatically) in patients with Takotsubo CMP.
- In addition — there is more-than-coincidental preceding occurrence of intense situational or psychological stress in many patients. This may be in the form of severe emotional stress (death of a loved one; break-up from significant other; overwhelming anxiety/depression) — pain — and/or fear (from earthquake or other catastrohic event). It is easy to understand the rationale for other names that have been used for this syndrome (ie, "Stress" Cardiomyopathy or "Broken-Heart" Syndrome).
- Although consensus is still lacking regarding specific criteria for defining Takotsubo CMP — there is general agreement that cardiac cath is diagnostic (ie, apical ballooning but no "culprit" artery).
SUMMARY of the Clinical Picture:
Takotsubo CMP is most typically seen in an older patient (most often in a post-menopausal woman) — who presents with chest pain or new heart failure. Look for the following features:
- Likelihood of preceding severe physical/emotional stress.
- Markedly abnormal initial ECG — often with diffuse ST elevation in inferior and antero-lateral leads (apical or LAD "wraparound" distribution). Associated T wave inversion and/or Q waves (sometimes deep) may be seen. Acute extensive STEMI-in-evolution is frequently the initial diagnosis (as it was in today's case).
- Usually no more than modest troponin elevation (troponins are often elevated — but generally not nearly as high as expected given how marked ECG changes are).
- Transient LV dysfunction — which may be severe initially (some patients present in pulmonary edema/cardiogenic shock requiring intra-aortic balloon pump support). LV function usually resolves within a few weeks.
- Possibility of potentially life-threatening arrhythmias during the acute phase (including VT/Torsades de Pointes).
- Absence of pheochromocytoma, myocarditis or other underlying cardiac pathology to explain findings.
- Generally favorable prognosis (often with full recovery within 1 month) — but fatalities have been reported (from LV free wall rupture; intractable pulmonary edema).
NOTE: Variations on the above theme do exist. The syndrome of Takotsubo CMP is not limited to post-menopausal women — the ECG does not always show marked abnormality — and severe stress does not uniformly precede presentation.
- Anatomic areas other than the apex may also be affected. For example — there may be an “inverted takotsubo” form, in which the apex is spared but the base of the heart is hypokinetic. The existence of such Takotsubo variants helps to explain the likely multifactorial etiology to this interesting syndrome.
PEARL: Think of the possibility of Takotsubo CMP when confronted with a patient who presents with a markedly abnormal ECG that doesn’t quite “fit” the clinical picture.
- ECG findings may be out of proportion to clinical findings. ECG changes may involve several lead areas (especially inferior and anterior precordial leads — which typically assess the cardiac apex).
- There may be an element of heart failure. Serum troponins may be positive.
- The patient is usually an older adult (especially a post-menopausal woman).
- There has usually been some form of severe preceding “stress”.
============================
ADDENDUM (1/2/2022):
I find it easy to forget about Takotsubo Cardiomyopathy. I've observed that many clinicians have a tendency to overlook this disorder. In the hope of serving as a helpful reminder — I've summarized in Figure-3 below, the ECG Findings that might be expected in Takotsubo Cardiomyopathy (adapted from Namgung in Clin Med Insights Cardiol).
 |
| Figure-3: ECG Findings in Takotsubo Cardiomyopathy (adapted from Namgung in Clin Med Insights Cardiol). |
- For another case of Takotsubo Cardiomyopathy — Please see the March 25, 2020 post in Dr. Smith's ECG Blog. Please check out My Comment at the bottom of the page!

.png)
