The lead II rhythm strip shown below in Figure 1 was obtained from an asymptomatic middle-aged adult. Is there complete (3rd degree) AV Block? How would you proceed clinically?
 |
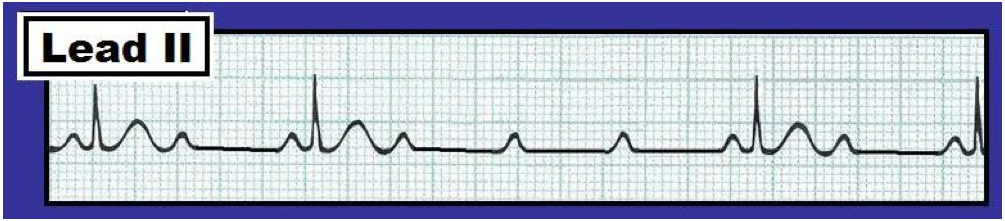
| Figure 1 - Lead II rhythm strip from an asymptomatic adult. Is there 3rd degree AV block? (Figure reproduced from ACLS-2013-ePub ). - Note - Enlarge by clicking on Figures - Right-Click to open in a separate window. |
INTERPRETATION: The ventricular rhythm in the Figure is regular at a rate just over 50/minute (since the R-R interval is slightly less than 6 large boxes in duration). The QRS complex is narrow, indicating a supraventricular etiology. P waves are present – however, they are not consistently conducting. Instead, the PR interval is changing. The PR interval preceding beats #3 and 4 (arrows) is clearly too short to conduct.
------------------------------------------------------
------------------------------------------------------
In ECG Blog #19 – we defined the 3 degrees of AV block as follows:
- 1st degree AV block – in which all atrial impulses are conducted to the ventricles, albeit with delay (so that the PR interval exceeds 0.20 second).
- 2nd degree AV block – in which some (but not all) atrial impulses are conducted to the ventricles.
- 3rd degree (or “complete”) AV block – in which none of the atrial impulses are conducted to the ventricles, despite having adequate opportunity for conduction to occur.
The key to the diagnosis of complete AV block is in the last part of the definition: No atrial impulses are conducted to the ventricles “despite having adequate opportunity for conduction to occur”. Although beats #3 and 4 in Figure 1 (and possibly also beat #2) are not conducted to the ventricles – none of these beats has a “chance” to conduct, since the PR interval is simply too short. Thus, we have no idea if any degree of AV block is present – since we cannot tell from Figure 1 if P waves could conduct were they given the opportunity to do so. We therefore interpret this tracing as showing “AV dissociation” – since at least some P waves are unrelated to the QRS complexes that follow them. The term AV dissociation should never be used as a “diagnosis” per se. Instead – it is the result of the underlying rhythm on the tracing. In this case – the underlying rhythm is sinus bradycardia at a rate of 50/minute (the P-P interval is precisely 6 large boxes in duration for each of the P waves on this tracing). AV dissociation occurs by “default”. That is – due to the relatively slow sinus rate, a nodal rhythm (at ~52/minute) takes over. This rhythm variant is not uncommonly seen in otherwise healthy young adult individuals. It may well be that there is no degree of AV block present, and that normal conduction will resume whenever the sinus node speeds up to a normal rate.
--------------------------------------------------
Distinction Beween AV Dissociation and Complete AV Block: In contrast to Figure 1 – the lead II rhythm shown in Figure 2 illustrates complete (3rd degree) AV block.
The atrial and ventricular rates in Figure 2 are both regular with no relation between P waves and neighboring QRS complexes. The QRS complex is wide, indicating AV block at the ventricular level. But the main distinction between Figures 1 and 2 is that despite more than adequate opportunity to conduct – none of the P waves in Figure 2 are conducted. We would not expect the P wave hidden in the T wave of beat #3 to conduct (because it occurs in the ST segment and is probably in the absolute refractory period). Similarly – the P wave preceding beat #1 in Figure 2 might not conduct (because this PR interval is not overly long). But virtually all other P waves on this tracing occur at a place when there should have been more than ample opportunity for conduction to occur. The diagnosis of complete AV block is therefore established.
 |
| Figure 2 - Lead II rhythm strip showing 3rd degree AV block. (Figure reproduced from ACLS-2013-ePub - pg 101) - Note - Enlarge by clicking on Figures - Right-Click to open in a separate window. |
--------------------------------------------

- See also ECG Blog Reviews #19, 20 – and Section 20.0 of our ACLS-2013-ePub -
--------------------------------------------