You are told that the
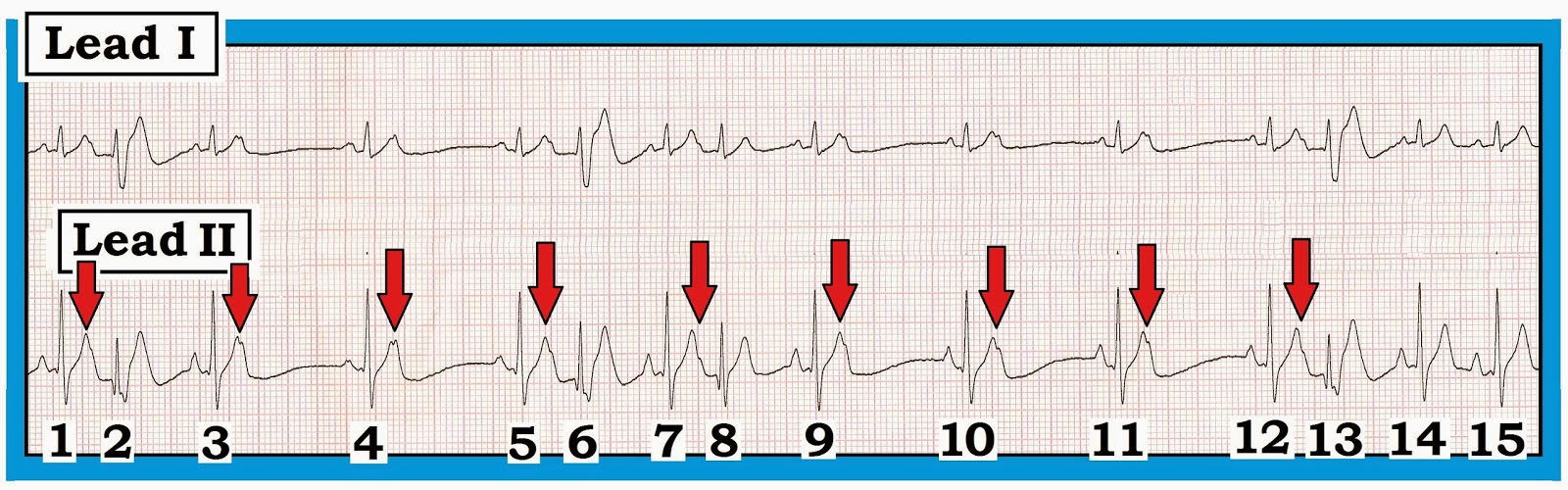
limb lead sequence shown in Figure-1
was obtained from a middle-aged adult. You note a Q wave and symmetric T wave inversion in lead III.
- Has this patient had an inferior infarction?
- Is T wave appearance in these 6 limb leads suggestive of ischemia?
 |
| Figure-1: Limb lead sequence from a middle-aged adult. Is lead III appearance suggestive of ischemia/infarction? |
Interpretation of Figure 1:
Clinical ECG interpretation is
dependent on history. It is essential to appreciate that ECG findings that
might prompt concern in a patient with new-onset
chest discomfort may not
necessarily be interpreted as abnormal in a non-acute
setting in an otherwise healthy individual. Such is the case for the 6 limb
lead sequence shown in Figure-1. We note the following:
- A Q wave is seen in lead III of Figure-1. Technically — this is a QS complex, since there is no R wave. Although this Q wave is not particularly deep (it is only 2mm) — given lack of any R wave, this Q wave (QS complex) portends the same clinical implications as would a larger or wider Q wave. That said — Q waves are not seen in the other 2 inferior leads (leads II,aVF).
- There is fairly deep symmetric T wave inversion in lead III (especially in view of the small amplitude for the QRS complex in this lead). IF this finding was noted in a patient with new-onset chest discomfort — We would clearly be concerned about acute ischemia. That said — there is no more than nonspecific ST-T wave flattening in lead aVF and no ST-T wave abnormality in the other inferior lead (= lead II ).
- Clinical Note: The T wave vector often follows fairly close behind the QRS vector. As a result — isolated T wave inversion that often occurs in leads III, aVL or aVF is clearly less likely to be ischemic IF the QRS complex is also predominantly negative in the lead that manifests T wave inversion. This is the case for lead III in Figure-1.
Impression: We would note the
following on our interpretation: “Q wave
with T inversion in lead III; nonspecific ST-T wave flattening in aVF; Suggest
clinical correlation”.
- That said — All bets would be off IF this patient had new-onset chest discomfort, since absence of abnormality in lead II does not exclude the possibility of acute ischemia/infarction. But IF this patient was asymptomatic (especially if a prior tracing was available and showed similar findings) — We would strongly suspect that the ECG appearance in lead III of Figure-1 was not indicative of ischemia/infarction.
- “Take-Home” Point: Most of the time when Q waves/T inversion reflects ischemia or infarction — neighboring leads will show similar changes.
Figure-2:
Normal Q Waves; Normal T Inversion
Among the most challenging tasks for
the ECG interpreter — is deciding what is “normal” vs “abnormal”. Our
purpose in devising Figure-2 —
is to facilitate remembering when the finding of even a large Q wave or deep
T wave inversion may be normal.
- 5 of the leads on a standard 12-lead ECG ( = leads III-aVR-aVL-aVF-V1) — may normally display even moderate-to-large Q waves and/or T wave inversion in healthy adults who do not have heart disease.
- Thinking of a “reverse Z” (à la Zorro) — may help to recall which leads these are (Figure-2).
 |
| Figure-2: Leads that may normally manifest T wave inversion or Q waves. Recall of these leads is facilitated by thinking of a reverse “Z”. |
KEY
Points:
Traditionally —
the finding of a deep and wide Q wave is thought to be a marker of myocardial
infarction. Other pathologic reasons
for Q waves exist — including cardiomyopathy (scarring/fibrosis); conduction defects and WPW. It is well to be
aware of instances when Q waves (and
associated T wave inversion) may be a normal
finding.
- Normal septal q waves — are common. Septal q waves are small and narrow. They arise because the first part of the ventricles to normally depolarize is the left side of the septum. As a result — left-sided leads see the initial depolarization vector as moving away from the left as the septum depolarizes from left-to-right. This accounts for the normal small q wave that may commonly be seen in one or more of the lateral leads (= leads I-aVL-V4-V5-V6) in asymptomatic individuals without heart disease. The reason we do not include normal septal q waves in Figure-2 is because their small and narrow dimensions makes it obvious that such q waves are unlikely to be pathologic.
- Lead aVR — is normally all negative (negative P wave, QRS and T wave — as seen in Figure-2). Global negativity for lead aVR is logical given the remote right-sided location of this unipolar lead (the depolarization vector continually moves away from right-sided lead aVR under normal circumstances).
- Lead V1 in adults — typically shows a QS or rS complex and T wave inversion (Figure-2). A QS complex may normally still be seen in lead V2 without this necessarily meaning there has been prior septal infarction. However, by lead V3 — at least some r wave should be seen under normal circumstances. Regarding T wave appearance in lead V1 — the T should normally be upright by lead V2 in adults. Persistent T wave inversion in anterior leads should prompt consideration of ischemia. NOTE: The situation is different in children — for whom anterior T wave inversion up to lead V3 (or even V4) may reflect a normal juvenile T wave pattern.
- Leads III, aVL, aVF (as in Figure-2) — may all normally show T wave inversion and/or an isolated Q wave that is not the result of ischemia or infarction — provided that these findings are not also seen in neighboring leads.
------------------------------------------
Applying Figure-2: Returning to Figure-1 — We see an isolated Q wave and T inversion in lead III. This may be a normal finding — especially IF: i) it is isolated to this single inferior lead (as it is in Figure-1); ii) the QRS complex in lead III is predominantly negative in the lead which shows T inversion; and, iii) the patient is not having new-onset chest pain.
Applying Figure-2: Returning to Figure-1 — We see an isolated Q wave and T inversion in lead III. This may be a normal finding — especially IF: i) it is isolated to this single inferior lead (as it is in Figure-1); ii) the QRS complex in lead III is predominantly negative in the lead which shows T inversion; and, iii) the patient is not having new-onset chest pain.
------------------------------------------
— For more information — GO TO —
- CLICK HERE — to download a pdf of Section 09.0 on ST-T Wave Changes (excerpted from ECG-2014-ePub).
- For additional Review on the Basics of assessing for Q-R-S-T Changes — lease see our ECG Blog #94 (Basic Concepts #7 ) -
- -
-
-- Please check out my Comment 1183 on the ECG Guru for additional illustration of how isolated findings in one of the above limb leads is generally "benign".
------------------------------------------