
QUESTION: Interpret the 12-lead ECG below.
- What type of conduction defect is present?
- Are ST-T waves doing what you'd expect given the presence of this conduction defect?
- Clinically - What else may be going on? (Is there LVH? - evidence of infarct?)
 |
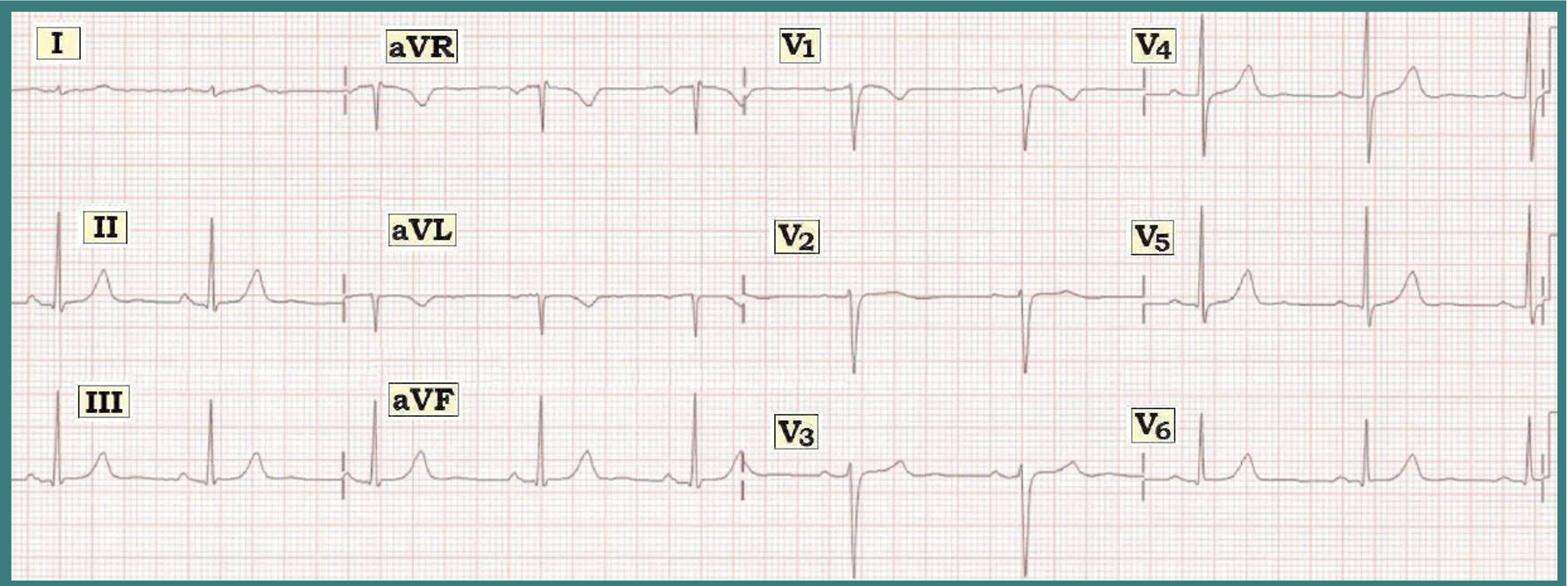
Figure 1: What type of conduction defect is present? |
INTERPRETATION: The rhythm is regular at a rate just over 100/minute. This qualifies the rhythm as sinus tachycardia at 102/minute. The PR interval is normal (ie, not more than a large box in duration). The QRS is obviously long. Recognition of QRS widening at this point is indication to STOP (and figure out WHY the QRS is wide) - before going any further:
- Assessment of QRS Widening: The 3 KEY leads to assess in order to determine the reason for QRS widening are leads I, V1, and V6. We look first at left-sided Leads I and V6 - which both show a wide monophasic R wave (albeit with slight slurring on the downslope in lead I). Right-sided Lead V1 shows an entirely negative QS complex. QRS morphology is therefore consistent with complete LBBB = Left Bundle Branch Block (See Figure 2 and LBBB Criteria below).
 |
Figure 2 - Typical Morphology for LBBB.
|
Criteria for LBBB (illustrated above in Figure 2):
- QRS widening to at least 0.12 second (whereas complete RBBB can occur with a slightly lesser degree of QRS widening = 0.11 second!).
- An upright (monophasic) QRS in leads I and V6 that may (or may not) be notched. But there should not be any q wave in either lead I or lead V6!
- A predominantly negative QRS in lead V1. There may (or may not) be an initial small r wave in lead V1 (lead V1 may show either a QS or rS complex).
Returning to Our Systematic Approach: The QT interval is less relevant in the setting of BBB (BBB by itself may prolong the QT). The axis is normal (close to 0 degrees) - albeit the concept of axis usually means little in the setting of BBB.
- Chamber Enlargement - There is probable LVH (See Impression below).
- Q-R-S-T Changes - There appears to be a Q wave in lead III. Otherwise - typical secondary ST-T wave changes are seen, consistent with the conduction defect (See KEY Rule and Figure 3 below).
------------------------------------
KEY Rule — Normally when there is typical RBBB or LBBB - the ST segment and T wave should be oriented opposite to the last QRS deflection in the 3 KEY leads (arrows in Figure 3). Deviation from this pattern in any of the 3 KEY leads (I, V1 or V6) is abnormal - and indicates a primary ST-T wave change (suggesting ischemia or infarction may be occurring).
 |
Figure 3 - ST-T Wave Changes Expected with BBB.
Note - The above KEY Rule for ST-T wave direction works only for RBBB and LBBB (but not for IVCD).
|
- In Figure 1 - ST-T waves are as expected for typical LBBB (ie, opposite to the last QRS deflection in each of the 3 KEY leads). Note that even the dramatic T wave peaking (with ST elevation) in anterior precordial leads of Figure 1 is as expected for LBBB. Lateral ST depression seen here is also not ischemic, but rather typical for LBBB.
CLINICAL IMPRESSION: We interpret this ECG as showing sinus tachycardia with complete LBBB - but no acute changes. Clinical correlation (and comparison with prior tracings) is needed to determine the significance of these changes, and whether they are new.
- It is always more difficult (but not necessarily impossible) to assess for ischemia and infarction when there is LBBB. Two important clues we routinely look for in this assessment are: i) the presence of typical secondary ST-T wave changes of BBB (See KEY Rule and Figure 3) - and ii) that no Q wave is seen in any lateral lead (there should be a monophasic R wave but no q wave with uncomplicated LBBB - as is seen in leads I, aVL, and V6 of Figure 1). The Q wave in lead III and the QS in lead V1 of Figure 1 are not indicative of infarction given the presence of BBB.
- Finally - It is also more difficult to assess for ventricular enlargement in the setting of LBBB. That said - the statistics are that many (if not most) patients with LBBB also have significant underlying heart diseasae (longstanding hypertension, heart failure, cardiomyopathy, coronary artery disease). By dint of their disease - many of these patients also have LVH (Left Ventricular Hypertrophy). The chance of true chamber enlargement with LBBB is extremely high (approaching 90%) - IF one finds very deep S waves (>25-30 mm) in leads V1, V2, or V3 and/or IF one finds LAA (Left Atrial Abnormality) in addition to LBBB. Given the appearance of Lead V2 in Figure 1 - we suspect there is probable LVH in this patient with complete LBBB.
--------------------------------------------------------
- See also ECG Blog Review #3 - and Review #13 -
- Please check out our ECG Video on Basics of Bundle Branch Block (www.bbbecg.com) -
--------------------------------------------------------
- See also ECG Blog Review #3 - and Review #13 -
- Please check out our ECG Video on Basics of Bundle Branch Block (www.bbbecg.com) -
--------------------------------------------------------













{kind=link}