
The ECG shown in Figure-1 was obtained from an elderly woman, who presented to the ED (Emergency Department) with an acute febrile illness (40°C).
- How would you interpret her initial ECG?
- Clinically — Could this be an early acute antero-septal STEMI?
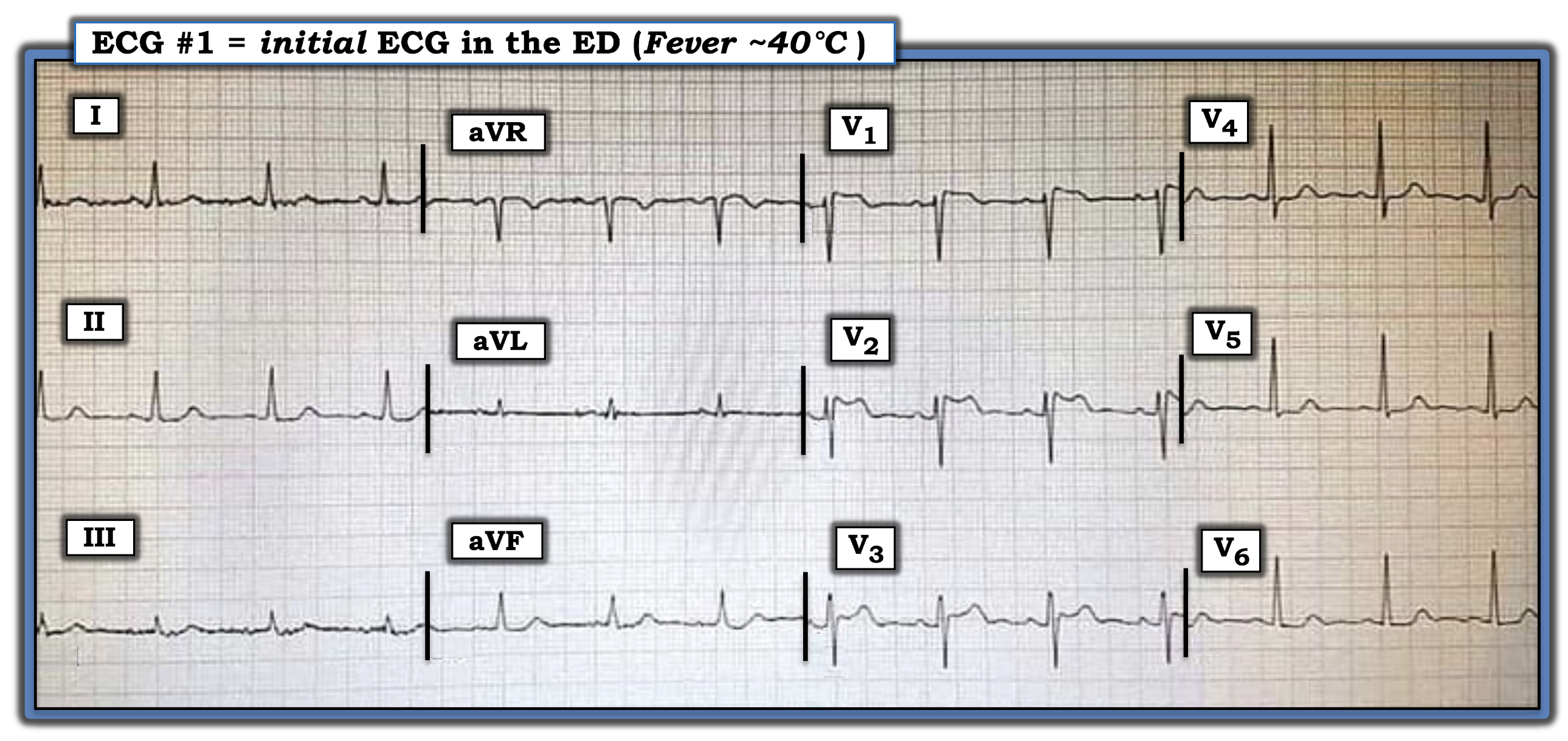 |
| Figure-1: ECG obtained from an elderly woman with an acute febrile illness (See text). |
The Case Continues:
The ECG was repeated (Figure-2) — this time with anterior leads placed 1 interspace higher.
 |
| Figure-2: Repeat ECG of the tracing shown in Figure-1, with anterior leads placed 1 interspace higher (See text). |
QUESTION:
- Do these serial tracings suggest an acute evolving anterior STEMI?
=======================================
NOTE: Some readers may prefer at this point to refer to ECG Media PEARL #53 before reading My Thoughts regarding the ECGs in Figure-2. This 2-part ECG Video (9 minutes and 8 minutes) — reviews the ECG recognition and clinical significance of Brugada-1 and Brugada-2 ECG patterns + it clarifies the concept of Brugada Phenocopy.
- For an excellent state-of-the-art Review article on Brugada Syndrome — CLICK HERE (Brugada J et al: J Am Coll Cardiol 72(9) 1046-1059, 2018).
- For a Review on the entity of Brugada Phenocopy — CLICK HERE (Anselm D et al: World Cardiol 6(3) 81-86-2014).
- For a study documenting the inability of experts to distinguish between a Brugada-1 ECG pattern from Brugada Syndrome vs Brugada Phenocopy — CLICK HERE (Gottschalk et al: Europace 18, 1095-1100, 2016).
- For brief summary of this material — Please refer to Figures-5, -6 and -7 in the Addendum below.
=======================================

=======================================
My THOUGHTS on this Case:
Looking first at the ECG in Figure-1 — The rhythm is sinus — all intervals (PR, QRS, QTc) and the axis are normal — and there is no chamber enlargement.
Regarding Q-R-S-T Changes in Figure-1:
- There are no Q waves.
- R Wave Progression is normal, with transition (where the R wave becomes taller than the S wave is deep) occurring normally between leads V3-to-V4.
- Regarding ST segments and T waves — the most striking abnormality is the ST elevation in leads V1, V2 and V3, with "double-hump" upward concavity in lead V3.
- ST segments are noticeably flattened in several limb leads — as well as in lateral chest leads (that also show slight ST depression).
My Impression of ECG #1: There is no denying the presence of anterior ST elevation with ST segment flattening and slight ST depression in other leads.
- That said — Against these ST-T wave changes in ECG #1 representing an acute cardiac event — is the clinical history of acute febrile illness in this elderly woman, with no mention in the history of associated chest pain.
QUESTION:
What happened in ECG #2 (bottom tracing in Figure-2)?
ANSWER:
The main difference between ECG #1 and ECG #2 is the appearance of the ST-T waves in leads V1, V2 and V3:
- The R' peak in leads V1 and V2 is higher in ECG #2, with sharp downsloping that leads into a more noticeably inverted T wave.
- The "double-hump" upward ST segment concavity that was seen in lead V2 of ECG #1 — is now seen in lead V3 of ECG #2.
My Impression of ECG #2: The ECG picture in Figure-2 stongly suggests we are seeing Brugada ECG patterns.
- The "double-hump" upward ST segment concavity in lead V2 of ECG #1 — is consistent with a Brugada-2 (ie, "Saddleback" ) pattern.
- The higher-rising, steeper downsloping ST-T wave appearance in leads V1 and V2 of ECG #2 — now meets criteria for a Brugada-1 ECG pattern, with a Brugada-2 pattern now seen in lead V3.
- In view of the clinical history — this is unlikely to represent an acute anteroseptal STEMI.
PEARL #1: It turns out that ECG #2 was repeated soon after ECG #1. This illustrates how the simple measure of placing anterior leads 1 or 2 interspaces higher on the chest may serve to bring out a Brugada ECG pattern!
The Case Continues:
The patient was treated for her acute febrile illness. Her ECG was repeated after her fever had resolved (Figure-3).
 |
| Figure-3: Repeat ECG following resolution of this patient's fever — compared to the initial ECG in this case (See text). |
QUESTION:
Does the patient in today's case have Brugada Syndrome?
WHAT is Brugada Syndrome?
First described in 1992 — the Brugada Syndrome is important to recognize because of an associated very high risk of sudden death in otherwise healthy young or middle-aged adults who have structurally normal hearts.
- The prevalence of Brugada Syndrome in the general population is ~1/2,000. The syndrome has become a leading cause of sudden death in young adults (under 40 years of age).
- PEARL #2: Brugada Syndrome is much more common in Southeast Asia compared to the rest of the world. When considering the possibility of this syndrome — demographics of the patient are important! (See Figure-6 in the Addendum below).
- PEARL #3: Although the genetics of Brugada Syndrome are complicated — the gender of the patient is also important. There is a distinct male predominance to this syndrome.
Personal Reflection: I never learned about Brugada Syndrome in medical school (the syndrome had not yet been described). But especially during the past 10 years, in which I've closely followed numerous international ECG internet forums — I've seen countless cases, especially of transient Brugada ECG patterns similar to today's case.
- Once a clinical entity is "discovered" — it begins to get noticed with increasing frequency.
Regarding BRUGADA Syndrome vs Phenocopy:
I reference an excellent state-of-the-art Review article on Brugada Syndrome (Brugada J et al: J Am Coll Cardiol 72(9) 1046-1059, 2018). I've synthesized key aspects of this article:
- A Brugada Type-1 ECG pattern is diagnosed by the finding of ST elevation of ≥2 mm in one or more of the right precordial leads (ie, V1, V2, V3) — followed by an r’ wave and a coved or straight ST segment — in which the ST segment crosses the isoelectric line and ends in a negative T wave (See Panel A in Figure-4).
- A Brugada-1 pattern may either be observed spontaneously (with leads V1 and/or V2 positioned normally — or — positioned 1 or 2 interspaces higher than usual) — or — a Brugada-1 pattern may be observed as a response to provocative drug testing after IV administration of a sodium-channel blocking agent such as ajmaline, flecainide or procainamide.
- NOTE: In the past, the diagnosis of Brugada Syndrome required not only the presence of a Brugada-1 ECG pattern — but also a history of sudden death, sustained VT, non-vasovagal syncope or a positive family history of sudden death at an early age. This definition was changed following an expert consensus panel in 2013 — so that at the present time, all that is needed to diagnose Brugada Syndrome is a spontaneous or induced Brugada-1 ECG pattern (without need for additional criteria).
- Panel B in Figure-2 illustrates the Brugada Type-2 or "Saddleback" ECG pattern. This pattern may be suggestive — but by itself, it is not diagnostic of Brugada Syndrome (See Figure-4).
 |
| Figure-4: Review of ECG Patterns in Brugada Syndrome (adapted from the above cited article by Brugada et al in JACC: Vol 72, Issue 9) — (A) Brugada-1 ECG pattern, showing coved ST-segment elevation ≥2 mm in ≥1 right precordial lead, followed by a negative T-wave. (B) Brugada-2 ECG pattern (the “Saddleback” pattern) — showing concave-up ST-segment elevation ≥0.5 mm (generally ≥2 mm) in ≥1 right precordial lead, followed by a positive T-wave. (C) Additional criteria for diagnosis of a Brugada-2 ECG pattern (TOP: the ß-angle; BOTTOM: A Brugada-2 pattern is present if 5 mm down from the maximum R’ rise point — the base of the triangle formed is ≥4 mm — as this ensures a ß-angle ≥58°). |
PEARL #4: A number of conditions other than Brugada Syndrome may temporarily produce a Brugada-1 ECG pattern. A partial list includes the following:
- Certain drugs (antiarrhythmics; calcium channel blockers; ß-blockers; antianginals; psychotropic medications; alcohol; cocaine; other drugs).
- Acute febrile illness.
- Variations in autonomic tone.
- Hypothermia.
- Electrolyte imbalance (hypokalemia; hyperkalemia).
- Ischemia/infarction.
- Cardioversion/defibrillation.
- Bradycardia.
KEY Point: Development of a Brugada-1 or Brugada-2 ECG pattern as a result of one or more of the above factors — with resolution of this Brugada ECG pattern after correction of the precipitating factor(s) is known as Brugada Phenocopy.
- The importance of being aware of this phenomenon of Brugada Phenocopy — is that correction of the underlying condition (ie, the acute febrile illness in today’s case) may result in resolution of the Brugada-1 ECG pattern — with a much better longterm prognosis compared to patients with true Brugada Syndrome (ie, an ICD may not be needed, as it probably would be if true Brugada Syndrome was present!).
- NOTE: To ensure a diagnosis of Brugada Phenocopy — the patient should have: i) A negative family history of sudden death; ii) Lack of a Brugada-1 ECG pattern in 1st-degree relatives; iii) No history of syncope, serous arrhythmias, seizures or nocturnal agonal respiration; and, iv) A negative sodium channel-blocker challenge test.
==================================
Final Comment on Today's Case:
Assuming the elderly woman in today's case had otherwise been healthy (without a personal history of syncope, serious arrhythmias, seizures or nocturnal agonal respiration) — the fact that the Brugada-1 ECG pattern we initially saw completely resolved so soon after fever resolution, strongly suggests she has Brugada Phenocopy (and not Brugada Syndrome) — and that her longterm prognosis is likely to be good.
- Whether she needs to undergo a negative sodium channel-blocker challenge test at her advanced age (and what impact her family history might have at her age) — are issues for her informed consent and medical providers to decide.
==================================
Acknowledgment: My appreciation to 유영준 (from Seoul, Korea) for making me aware of this case and allowing me to use this tracing.
==================================
References & Related ECG Blog Posts to Today’s Case:
- For an excellent state-of-the-art Review article on Brugada Syndrome — CLICK HERE (Brugada J et al: J Am Coll Cardiol 72(9) 1046-1059, 2018).
- For a Review on the entity of Brugada Phenocopy — CLICK HERE (Anselm D et al: World Cardiol 6(3) 81-86-2014).
- For a study documenting the inability of experts to distinguish between a Brugada-1 ECG pattern from Brugada Syndrome vs Brugada Phenocopy — CLICK HERE (Gottschalk et al: Europace 18, 1095-1100, 2016).
- ECG Blog #50 — For a case of Brugada Syndrome.
- The September 5, 2020 post in Dr. Smith's ECG Blog (Please scroll down to the bottom of the page to see My Comment). This case shows an example of Brugada Phenocopy as a result of Hyperkalemia.
- The May 6, 2019 post in Dr. Smith's ECG Blog (Please scroll down to the bottom of the page to seeMy Comment). This case reviews an example in which it was difficult to distinguish between Brugada Phenocopy vs an ongoing acute STEMI.
- The September 8, 2019 post in Dr. Smith's ECG Blog (Please scroll down to the bottom of the page to see My Comment). This case reviews another example of Brugada Phenocopy as a result of Hyperkalemia.
==================================
ADDENDUM (7/1/2021): Summarizing material on Brugada Syndrome:
 |
| Figure-5: 2-page Summary of the essentials of Brugada Syndrome (from my ECG-2014-ePub). |
 |
| Figure-6: World prevalence map of Brugada Syndrome. The overall worldwide prevalence of Brugada Syndrome is ~0.5/1,000 in the population. This prevalence is highest in Southeast Asia (at least 5 times more common than in North America). The country with highest prevalence of Brugada Syndrome is Thailand, with ~15 times higher prevalence thn the worldwide average. Brugada-2 patterns (ie, "Saddleback") are also much more prevalent in Southeast Asia than elsewhere in the world. (Excerpted from Vutthikraivit et al: Acta Cardiol Sin 34:267-277, 2018). |
 |
| Figure-7: Summarizing Figure of KEY concepts reviewed in the above ECG Videos (ECG MP-53). |
Very well explained. Thanks
ReplyDeleteMG
My pleasure! — :)
DeleteMillions thanks to Ken for this wonderful case presentation and lesson. I cannot be more grateful than this 🙂
ReplyDeleteMy pleasure! — :)
Delete