
- How would YOU interpret the ECG in Figure-1 ?
- Is this history helpful for making the diagnosis?
-USE.png) |
| Figure-1: The initial ECG in today's case. (To improve visualization — I've digitized the original ECG using PMcardio). |
- #1) Does the rhythm need immediate treatment? (as might be the case if the rhythm was excessively fast or slow).
- #2) IF the patient is hemodynamically stable and the rhythm does not need immediate treatment — I then take a brief look at the rest of the 12-lead ECG.
- The QRS in Figure-1 is obviously wide (clearly more than half a large box in duration).
- The ventricular rhythm is almost (but not completely) Regular — in that R-R intervals vary between being a little more or a little less than 5 large boxes in duration.
- The Rate of the rhythm is ~60/minute (300 ÷5 ~60/minute).
- Some P waves are present! That said — we do not see P waves throughout the entire tracing.
- The P waves that we do see, do not appear to be Related to neighboring QRS complexes (because the PR interval looks to be continually changing).
- We do not yet know about this patient's hemodynamic status. That said — a wide QRS rhythm at a rate of ~60/minute (even if this represents 2nd- or 3rd-degree AV block) — usually does not need immediate treatment.
- PEARL #1: As noted above — the QRS complex is wide. Whenever we detect that the QRS is wide — we want to determine as quickly as possible WHY is the QRS wide?
- Is QRS widening the result of some form of bundle branch block?
- — OR — Is this a ventricular rhythm?
- Why did YOU think the QRS is wide in Figure-1?
- #1) There is a supraventricular rhythm with some type of conduction disturbance (due to either aberrant conduction or preexisting bundle branch block). As reviewed in ECG Blog #204 — there are 3 basic types of conduction disturbances ( = RBBB, LBBB and IVCD).
- #2) There is WPW.
- #3) There is a ventricular rhythm.
- #4) There is some type of "toxicity" causing QRS widening.
- WPW is not present — as P waves are not conducted, and there are no delta waves.
- Aberrant conduction is most often seen in association with a rapid ventricular rate — and the heart rate here is not fast.
- QRS morphology does not resemble any known form of conduction disturbance (ie, There is no upright QRS in lead V1, as would be the case with RBBB — and the QRS is essentially all negative in all 3 inferior leads and in all 6 chest leads). This strongly suggests a ventricular rhythm.
- QUESTION: Did YOU notice peaking of T waves?
- ST-T waves look overly peaked (if not pointed) in multiple leads (ie, in leads II,III,aVF; and V3-thru-V6). The size of many of these T waves looks to be disproportionately increased with respect to the size of S waves in these leads.
- My Impression: This patient is almost certain to have significant Hyperkalemia — so much so, that I’d empirically give IV Calcium, even before knowing what the serum K+ level is.
- My discussion of a similar case in ECG Blog #275 reviews the textbook description for sequential ECG changes seen with progressive degrees of hyperkalemia. But many patients do not read the textbook — such that any sequence of ECG changes may be seen (including cardiac arrest prior to T wave peaking and QRS widening).
- Increased K+ release from cells as a result of injury sustained during surgery.
- Reduced urine output/acute renal insufficiency.
- Hypovolemia (that may have been present before surgery — or developed during surgery).
- Exogenous K+ load (ie, from blood transfusions).
- Rhabdomyolysis (from malpositioning of the patient during surgery).
- Use of K+-retaining medications just before or during surgery.
- Acidosis (which promotes redistribution of K+ from intracellular to extracellular compartments).
PEARL #3: Rapid recognition of Hyperkalemia is among the most important of skills for emergency providers to master. The reasons for this are simple:
- i) Hyperkalemia is potentially life-threatening.
- ii) There is an empiric treatment (ie, IV Calcium) that can be life-saving — and which should sometimes be given prior to lab confirmation of hyperkalemia. Cautious administration of IV Calcium is safe — and, not-to-promptly treat the patient risks losing the patient.
- iii) Not-to-recognize hyperkalemia as the cause of QRS widening, unusual rhythm disturbances and/or ST-T wave abnormalities — will lead you down the path of potentially serious misdiagnosis.
PEARL #4: Considerations regarding use of IV Calcium:
- IV Calcium works fast (ie, within 2-3 minutes) by an action that stabilizes myocardial membrane potential, thereby reducing cardiac membrane excitability provoked by hyperkalemia (and thereby protecting against cardiac arrhythmias). NOTE: IV Calcium does not cause intracellular potassium shift, and it does not facilitate elimination of this cation.
- Either Calcium Chloride or Calcium Gluconate can be used (10 mL given IV over 3-5 minutes with ECG monitoring). NOTE: The chloride form contains 3X the amount of calcium per 10 mL dose (10 ml 10% CaCl = 6.8 mmol Ca++ vs 10 ml 10% CaGlu = 2.3 mmol Ca++).
- IV Calcium should be repeated IF there is no effect (ie, narrowing of the QRS on ECG) after 5-10 minutes. More of the gluconate form may need to be given (since it contains less calcium).
- The duration of action of IV Calcium is only ~30-60 minutes — but this is more than enough time to allow other treatments to work.
- CaGlu can be given through a peripheral IV line. Because CaCl is more likely to cause tissue necrosis if there is extravasation — a central line is recommended (except if your patient is in cardiac arrest).
- Other treatments will often be needed (ie, Glucose/Insulin; Albuterol inhalation; Sodium Bicarbonate — and in refractory cases, hemodialysis) — but IV Calcium is the initial treatment of choice for life-threatening hyperkalemia.
- NOTE: IV Calcium is not indicated for the treatment of peaked T waves with a narrow QRS and reasonable rhythm — as this is not a life-threatening situation.
PEARL #5: Assessment of the rhythm with severe hyperkalemia is often difficult for several reasons (as summarized below in Figure-2):
- As serum K+ goes up — P wave amplitude decreases. Eventually — P waves disappear.
- As serum K+ goes up — the QRS widens.
- In addition to bradycardia — any form of AV block may develop. Therefore — Think of hyperkalemia in the presence of any bradycardia when the QRS is wide (even if there is no T wave peaking).
- Cardiac arrhythmias that develop in association with severe hyperkalemia often "do not obey the rules" — such that identification of a specific rhythm diagnosis may not be possible in patients with severe hyperkalemia.
- ANSWER: The ECG will look like there is a ventricular escape rhythm — or — like the rhythm is VT if the heart rate is fast.
PEARL #6: As we have just noted, with progressive hyperkalemia — P wave amplitude decreases until ultimately P waves disappear.
- Interestingly — the sinus node is often still able to transmit the electrical impulse to the ventricles in such cases, even though no P wave may be seen on ECG. This is known as a sinoventricular rhythm.
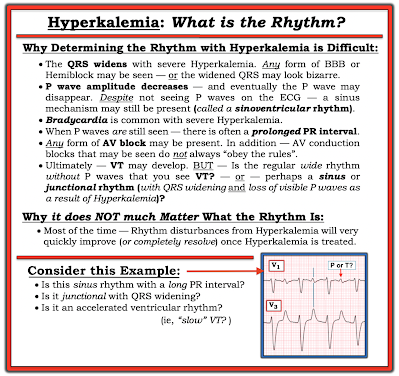 |
| Figure-2: Why assessing the rhythm with hyperkalemia is difficult. |
PEARL #7: In my opinion, it is not worth wasting time trying to figure out the specific rhythm diagnosis of a bradycardia when there is hyperkalemia. I used to spend hours trying to do this — but after years of doing so, I finally realized the following:
- i) That a specific rhythm diagnosis may not be possible when there is significant hyperkalemia — and, even if you succeed in making a diagnosis such as Wenckebach — chances are as serum K+ intra/extracellular fluxes change, that the cardiac rhythm will also soon change; and,
- ii) Clinically — it does not matter what the specific rhythm diagnosis is once you recognize hyperkalemia that needs to be immediately treated — because usually within minutes after giving IV calcium, the "bad" rhythm will most probably "go away" (often with surprisingly rapid reestablishment of sinus rhythm).
==============================
What about the Rhythm in Today's CASE?
Let's return to today's ECG. We determined in Figure-1 (that I reproduce below) — that the rhythm is fairly (but not completely) regular, at an average rate of ~60/minute — with at least some P waves, albeit these P waves do not appear to be related to neighboring QRS complexes.
- KEY Point: QRS morphology in Figure-1 does not resemble any known form of conduction defect (ie, the all-negative QRS across the 6 chest leads suggests that the wide QRS represents a ventricular rhythm).
- Are there additional P waves that are hidden in Figure-1?
|
| Figure-1: I've reproduced the initial ECG in today's case. |
- Set your calipers to this P-P interval suggested by the distance between 2 consecutive RED arrows.
- Note in Figure-3 — the partially hidden PINK arrow P wave that precedes the 4th and 5th RED arrow P waves. These last 3 colored arrows suggest what the P-P interval might be for a fairly (but not completely) regular underlying sinus rhythm.
-labeled-P-USE.png) |
| Figure-3: I've identified those P waves that we definitely see ( = the RED arrows). To this, I've added a PINK arrow for what appears to be a partially hidden P wave. |
-labeled-maybe-USE.png) |
| Figure-4: Colored arrows suggest an underlying sinus arrhythmia. |
- That said, when AV block is truly "complete" — the ventricular escape rhythm tends to be more regular than what we see in Figure-4. Most of the time — QRS complexes that appear earlier-than-expected are the result of some conduction (therefore 2nd-degree instead of 3rd-degree AV block).
- BOTTOM Line: None of this matters clinically! It is simply not worth wasting time trying to distinguish between 2nd-degree vs 3rd-degree AV block in Figure-4 — because arrhythmias often "do not obey the rules" when there is significant hyperkalemia — and the rhythm will probably normalize within minutes of giving IV Calcium.
==================================
Acknowledgment: My appreciation to Ahmed Marai, Safen Haider, and Zahraa Ali (from Iraq) — for allowing me to use this case and these tracings.
==================================

Interesting and well explained, I just have few questions
ReplyDelete1. Why did we say that the QRS widening is because of the ventricular rhythm, not because of the hyperkalemia?
2. If the patient was unstable, would you start pacing + calcium? Or how would you approach it?
Thanks again!
THANK YOU for your comment! There is a lot of "semantics" in this — as I suggest in Figure-2 and in Pearl #7 — simply because markedly hyperkalemic patients often "do not read the textbook". By this I mean that they can get almost any arrhythmia — and the usual "rules" for interpreting the specific type of AV block don't apply. As for wide rhythms — it's often hard to distinguish between a ventricular rhythm vs loss of P waves and a wide QRS strictly from the hyperK. In this case — the AV dissociation tells us the QRS is wide because it is a ventricular rhythm.
DeleteSo to answer your question #1 — the ventricular rhythm is the result of hyperK — but then again, none of this truly matters because IV Ca++ should treat both the ventricular rhythm and the hyperK.
As to what to do if the patient is unstable — Sometimes, "Ya gotta be there". If at all possible, immediate administration of IV Ca++ may be all that is needed (and you can repeat the IV Ca++). But if bradycardia persists — then pacing may be needed. THANKS again for your comments — :)